A Next Einstein Forum opinion paper
Since the first case of the novel coronavirus (2019-nCoV), was detected in Wuhan, China, towards the end of 2019, and declared a global pandemic on 11 March by the World Health Organization, attention has now turned to how countries have responded. The magnitude of the resultant shock from COVID-19 has tested healthcare and disaster management systems of countries and the agility of policy responses to a public health catastrophe.
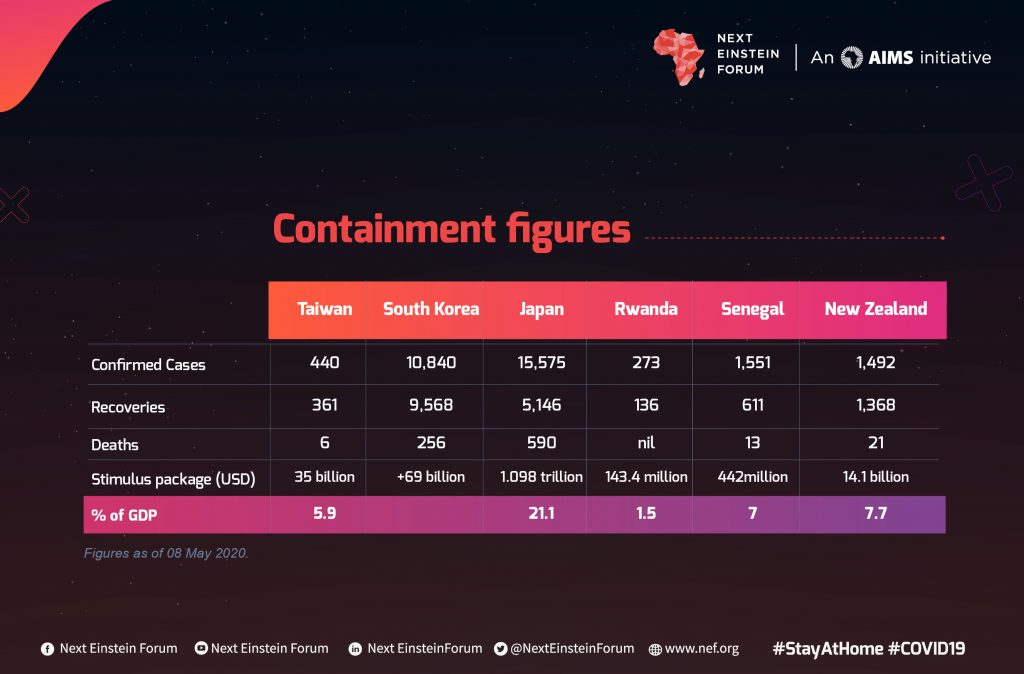
As of 8 May, 212 countries and territories worldwide had confirmed cases of COVID-19. In Africa, the disease was first confirmed in Egypt on the 14th of February followed by Algeria and Nigeria two weeks later, with all cases being imported via air travel. A total of 57,846 confirmed cases, 2,126 resulting deaths and 19,359 recoveries (as of 8 May) have been reported in 53 African countries. Although many countries are still grappling with the disease, fighting to inverse the infection curve, there is a flicker of hope from other countries that have managed to contain the disease with varying levels of success.
Taiwan, South Korea, Japan, Norway, New Zealand, Rwanda and Senegal have taken varying approaches to prevent and manage the spread of the virus, reducing negative effects on their citizens. This opinion paper seeks to review their responses and draw lessons for African countries.
Five Asian countries– Japan, South Korea, Hong Kong, Singapore and Taiwan have had only 876 deaths combined by 8 May, despite their proximity to China. This phenomenon is now being referred to as the “New Asian Miracle.” These countries are part of a region that has grappled with other acute respiratory infections such as SARS and MERS, also caused by types of human coronaviruses. Their responsiveness to the novel coronavirus can be attributed to the experience gained from managing similar outbreaks in the past.
African countries who registered cases well into February have also been early responders. Almost all countries have instituted partial or full lockdown, limiting movement both externally and internally. Nigeria was the first to report the SARS-CoV- 2 genome sequence from Africa on 4 March. South Africa is now leading the continent in testing per capita (5,189 tests/million people as of 5 May). At the beginning of April, Kenya had converted existing factories into mask production. Almost all African countries, from Egypt to South Africa are building affordable ventilators and using digital and emerging technologies for tracking and other economic activities. This has been accelerated by the breakdown of supply chains and the need to look inwards.
This opinion paper will pull out the successful interventions in various country responses and then propose recommendations for African countries for this and future pandemics.
1. Taiwan: Overall strategy
Taiwan was in the hot zone with an estimated second-highest importation risk due to its proximity to China and the strong socio-economic and cultural interactions between the two countries. Using experience from previous outbreaks, Taiwan quickly activated its emergency response team soon after WHO announced the presence of a new coronavirus in Wuhan, China. Taiwan is not a member of the WHO but responded swiftly and continues to flexibly benefit from the work of the organization. The Taiwanese government started screening for 26 viruses including SARS and MERS and quarantined travelers coming in from Wuhan. This was later extended to include all inbound Taiwanese travelers while placing an entry ban on foreign nationals.
Taiwan’s first confirmed case of COVID-19 was announced on 21 January and by 8 May, 440 confirmed cases, 6 deaths and 361 recoveries were reported. Taiwan had conducted 2,807 tests/per million people, comparatively much lower than the United States’ (US) 26,099 tests/million people. However, the magnitude of the outbreak is more than 200 times bigger in the US than in Taiwan (18 cases/million against US’ 3,994 cases/million) therefore, Taiwan has conducted more testing relative to the size of the outbreak. The low number of infections, more than 60 days after the initial case was discovered, attests to Taiwan’s well-functioning and inclusive health system which has a 99% coverage rate for health insurance. Remarkably, the Taiwanese government merged health insurance, immigration and customs databases to identify, track and trace contacts, monitor cases and make appropriate interventions for each case. This was largely enabled by applying emerging technologies such as AI and Big Data analytics.
Instead of a lockdown, Taiwan resorted to isolation, quarantine and self-management of suspected cases, which were strictly monitored through mobile phones. To avoid panic, the government focused on transparent and frequent communication. With a highly competitive science and innovation ecosystem, Taiwan became the 4th country in the world to come up with a pure strain of COVID-19 and developed a rapid immune-based diagnostics kit that is able to identify COVID-19 antibodies in less than 20 minutes. In a nod to agility, the government established a task force with a mandate to ensure the swift regulation of the new technologies. The Taiwanese government released a US$34.64 billion economic stimulus package. The government also intervened to support the industry by injecting US$6 million to create 60 new mask production lines, increasing capacity from 1.8 million to 8 million masks daily, each mask costing about US$0.17. Furthermore, Taiwan donated 10 million masks to the US, Spain, Italy and other European countries as a medical diplomacy gesture.
In Africa, Kenya has also engaged in mass production of masks since the beginning of April targeting tens of millions in production. The Kenyan government made masks mandatory in public spaces on 4 April. Others quickly followed.
- South Korea: Test, track, self-isolate
South Korea reported its first confirmed case on 20 January and was on case 31 by 18 February. The highest spike in confirmed cases occurred on 29 February, recording 909 infections in a single day. As of 8 May, the total number of confirmed cases was 10,840 (including 688 imported cases), 9,568 recoveries, 256 deaths and 1,016 active cases. Despite the high risk of importation due to proximity to China, South Korea has been commended for containing the spread of COVID-19, though the likelihood of resurgence is high.
Organizational memory from the MERS epidemic played a pivotal role in the decisions leading to the adoption of the approach taken. As of 8 May, testing stood at 12,874 tests/million people. South Korea’s approach focuses on extensive testing, isolation and tracking of infected people followed by tracing and quarantining contacts using digital surveillance. These are very intrusive measures, but gained social acceptance which might have played out differently in western countries. South Korea innovatively came up with 43 drive-through testing stations and public “phone booths” which have since been replicated in other countries. These testing strategies increased testing capacity by 10 times. As of 2 April, they had managed to bring down the number of new cases to 100 a day from the earlier peak of 909 cases. South Korea did not opt for a complete lockdown, focusing instead on partial lockdown of infection clusters.
Finally, as an incentive and to cushion its citizens, the Korean government is giving people who are self-isolating including those who are yet to test positive 454,900 won a month (about US$374) to cover basic living expenses. The Korean recently added US$69 billion to the economic stimulus package which covers a range of applications. South Korea contributed about US$170 million towards vaccine development and has pledged to support partner countries to build capacity in infectious disease response.
- Japan: Containment by Cluster Countermeasures &Social distance as culture
Japan was one of the first countries outside of China to discover novel coronavirus cases, direct imports from Wuhan on 16 January. Japan eventually declared a state of emergency implemented in stages, starting with 7 prefectures including Tokyo and Osaka on 7 April and later extended on 16 April to cover the whole country. However, governors in each prefecture get to decide the type and level of measures they can enforce to contain the outbreak. Despite the declaration, 60% of employed people are reported to still be commuting to work. On 17 April, Tokyo broke the 200 mark of daily infections, recording 201 new infections in a day. As of 8 May, Japan had reported 15,575 confirmed cases, 590 deaths and 5,146 recoveries.
Japan has been criticized for taking a somewhat relaxed approach to containing the spread of COVID-19 despite having a very high risk of importation and an elderly population that is more vulnerable to the virus. However, as of 9 March, analysis shows that 80% of the confirmed cases had not passed the infection to anyone which points to successful transmission containment. The country’s strategy was hinged on early detection of and early response to clusters. To qualify for testing one had to meet stringent conditions set by the government to concentrate care on those with severe symptoms to avoid clogging the health system. The government also made use of alternative testing methods such as using CT scanners to identify pneumonia and treat without conducting COVID-19 tests. As well, to improve the rate of diagnosis, Nagasaki University in partnership with the government and a private firm created a test kit that can produce results within 10 minutes. Studies and other discourse points to the general habit in Japan, and other parts of Asia, of wearing masks and limited skin to skin contact (“skinship”) even during periods outside of COVID – 19 as contributing to the early containment. The use of masks is believed to have contributed to the remarkable drop of flu infections within 7 weeks of the start of the coronavirus outbreak. Also, citizens were instructed to avoid crowds, poorly ventilated spaces and close proximity to others.
On the economic side, the Japanese government issued emergency response packages targeted at the healthcare system, child care and MSMEs (Micro, Small and Medium-Sized Enterprises) and recently added a stimulus package of 108 trillion yen (about US$990 billion). A handout of 100,000 yen (about US$930) will be distributed to individuals on the basic resident register including the homeless and foreigners beginning May 2020 following cabinet deliberations, the handout package amounts to a total of about 12.8 trillion yen.
- Rwanda: Digital tools for prevention
Rwanda recorded its first case on the 14th of March after 900 tests at a daily rate of 20-30 tests. Findings from the initial contact tracing revealed the first 17 cases had contact with about 680 people. The Rwandan government was proactive in closing schools early. They also dispatched trained officials to border posts to conduct screening and established handwashing stations at bus stations in the capital city and enforced a 14-day quarantine at designated places for all inbound travelers. The Rwandan government eventually declared a total lockdown on 21 March extended to 30 April, prohibiting intercity travel, between urban and rural areas and all non-essential movement outside homes (including an outright ban on public transport).
Rwanda has encouraged digital money transactions and online shopping to minimize the risk of transmitting the virus through cash transactions. On 26 April, the government launched a permission system that allowed residents to request permission to leave their homes for essential services online or via USSD messaging. Police officers throughout the country can quickly check if permission is granted via mobile or tablet by inputting car plate numbers or telephone numbers. Finally, with the upsurge of infections of cross-border truck drivers, Rwanda implemented a relay system, with trucks offloading and customs related transactions happening at the border points directly. Rwandan drivers are then required to move the cleared loads from the border into the country.
To curtail the economic impact of COVID-19, Rwanda, among several other African countries, is set to benefit from the World Bank’s $2 billion programme and receive further support through the Rwanda COVID-19 Emergency Response project. Rwanda is receiving an additional US11 million dollars in debt relief from the IMF. The government of Rwanda has come up with an Economic Recovery Plan (May 2020-December 2021) with a total budget of about FRW134 billion (US$143.4 million). On the humanitarian front, Rwanda has taken the lead in providing food and groceries to its vulnerable people during the lockdown period. The government of Rwanda continues to intensify its awareness efforts through the use of drones, which are also being used in Ghana to deliver COVID-19 test samples. As of 8 May, Rwanda had a total of 273 cases out of which 136 recovered and zero deaths.
- Senegal: Clear treatment plan and agile innovation
Senegal confirmed its first case on 2 March and by 8 May, the number of confirmed cases had risen to 1,551 with 13 deaths and 611 recoveries. The Health Emergency Operations Center (HEOC) was activated on the day that the first case was discovered, receiving funding, equipment and technical assistance from the US Defense Threat Reduction Agency. The country has since declared a State of Emergency, closed schools, suspended flights, banned public gatherings and placed a curfew alongside the basic prevention guidelines stipulated by WHO. Screening booths were established at ports of entry such as airports and a rapid response team was put on standby to get to the sick persons and take samples. The government faced some resistance in the initial phases over closures of worship centers which indicates the need for wide consultations for greater buy-in from all sectors. Marked differences in infection rates between urban and rural areas have been observed in Senegal. The largely rural Matam and Kaffrine regions have not been affected yet while the capital city, Dakar, accounts for 60% of COVID-19 infections. Similar trends have been observed across Africa.
Notably, Senegal has experienced a relatively high rate of recovery, reaching 61% recovery at some point. The country has been making use of treatment regimens that seem very promising and is planning on trying out herbal remedies (COVID-Organics) from the Artemisia plant working with the government of Madagascar[1]. In addition, researchers at Institut Pasteur in Dakar are collaborating with a UK-based company to develop an immune-based diagnostic test for COVID-19, which can be done at home and can produce results within10 minutes at an affordable cost of only US$1.The team is hoping that after navigating the regulatory process, the test kits can be deployed across Africa.
On the economic side, the government established a national solidarity fund to support firms and households worst affected by COVID-19 and is using part of the funds to upgrade the health system in preparing more clinics. In addition, the technology sector has rallied to create a tracking application to help the government to track distributions of food and personal protective equipment. Senegal is set to receive about US$221 million to offset the negative impacts of the COVID-19. On 2 April, The World Bank approved a $20 million credit to support Senegal as part of the national COVID-19 response plan which includes financing, policy advice and technical assistance.
- New Zealand: Decisive,science-informed leadership
With a strategy to eliminate the new coronavirus, New Zealand opted to go for the strictest measures first (Alert Level 4), and then de-escalate as the situation improves. Prime Minister Jacinda Arden was applauded for her swift response, empathy, responsiveness to scientific advice and great communication skills which enabled her to gain public trust. Her decisive leadership started the debate on the successful response of female leaders globally.
The total lockdown was enforced on 23 March. New Zealand detected its first case a full two months after the first case of coronavirus was discovered in Wuhan. The country’s remote location and geography could be a contributing factor but New Zealand should be commended for its decisive leadership and swift action. New Zealand is relatively small with a population of about 4.8 million people but can get up to 4 million tourists a year, making it very vulnerable to global outbreaks such as the novel coronavirus.
As of 8 May, New Zealand had 1,492 confirmed cases, 1,368 recoveries and 21 deaths, from a total of 183,039 tests (37,957 tests/million people). Of the confirmed cases, 2 are hospitalized with no cases in ICU. The country is showing an impressive recovery rate – so far the number of recovered cases is higher than active cases. Initially, testing was targeted to people showing symptoms. From 16 April, testing was expanded to include the asymptomatic through random voluntary community testing in places such as supermarkets. To date, the government has identified 16 significant clusters[2] and continues to monitor those, 4 of which were closed by 8 May. The country has since de-escalated to Alert Level 3 -Restrict beginning 28 April.
The lockdown affected consumer and leisure activities dropping by 88%. In response, the New Zealand government announced a NZ$23 billion stimulus package (7.7% of GDP) (about US$14.1 billion), making a 12-week advance payment to businesses and workers. Furthermore and in an act of solidarity, the Prime Minister of New Zealand together with her cabinet cut their pay by 20% in the next 6 months and the leader of the opposition also followed suit. On the other hand, the government released funding through the Medical Research Institute of New Zealand to co-lead internationally significant trials that will assess the efficacy of potential treatment agents such as hydroxychloroquine. Finally, New Zealand, like many countries globally, is running a dedicated website for COVID-19 where information is shared in real-time and all important updates and documents can be easily accessed.
Key Learnings
South Korea, Taiwan and Rwanda responded to the public health threat early and have focused on testing, tracking and isolating. On the other hand, Japan and Senegal have concentrated resources on testing and treating the infected with Senegal showing impressive agility in leveraging innovation.
We have made sure to highlight the economic stop-gap and stimulus responses which are critical if a public health response is to succeed. The two must go hand in hand. We also believe decisive political leadership is critical to accelerating containment and recovery. The question of the importance of female leadership is one that needs further unpacking but it is clear that in places with feminist leadership, effective containment measures and clear public engagement has been observed.
So, what can other countries do in the immediate to avert the effects of COVID- 19? How can they prepare for future shocks of the same magnitude, whether it be a public health crisis or a natural disaster? Several important lessons can be gleaned from the interventions taken by these various governments. We recommend the following strategies are adopted contextually:
- Vision and Funding for Research and Development (R&D) in Africa
- African countries need to adopt a common vision and strategy for research and development which results in the establishment of funding mechanisms for implementation from research to industrialization.
- Governments, Pan-African and development actors must establish and fund a Pan-African data-driven knowledge ecosystem to assist government agencies to derive better insights for critical decision making to produce more agile responses in terms of policies, interventions and resource allocation.
- During a crisis, there must be mechanisms to call for, fund, regulate a portfolio of digital and emerging technology tools that local and national governments could customize and deploy.
- More centers of excellence and regional laboratories must be established to produce technical experts ready to solve local problems with additional agile funding for pandemics.
- There needs to be systematic funding to the African Centre for Disease Control and other regional pandemic initiatives.
- Promote multiple helix partnerships. These relationships are key to unlock innovative capacity across sectors. Institut Pasteur in Senegal, Nagasaki University in Japan and the Mask Industry in Taiwan exhibit how effective these relationships like these can help churn out innovations of high commercial value. However, these interlinkages require coordination at the central level and demand finding innovative and appropriate funding instruments to support such partnerships.
- Invest in science/health diplomacy. African countries should actively participate in science and health diplomacy and consider collectively or individually contributing to global funds, innovations and/or expert councils. Taiwan donated masks; South Korea shared expertise on health response while New Zealand, Norway and Japan donated funds to global clinical and humanitarian initiatives. African countries should make sure that African researchers are sitting on these global panels, and providing contextual advice to both global and local decision-makers. This is also critical for solidarity trials and how African countries participate.
- Early Response Mechanisms
- Adopt early medical response
- Countries should adopt a screen, test, and treatment response as early and for as many people as possible, optimizing resources. Here, mechanisms to minimize regulatory hurdles should be put in place to allow experimentation and agility in implementation particularly leveraging informed use of technology.
- Quickly activate existing systems. South Korea, Japan and Taiwan adopted different strategies to contain COVID-19. Their relative success in keeping the rate of infections and the number of deaths low is largely hinged on the organizational memory obtained from past SARS and MERS pandemics. Some African countries, like Nigeria and Senegal, have also built resilience by responding to Ebola, Lassa fever and Dengue outbreaks. Many countries do not have a fully developed emergency response plan thus going forward; African countries will need to concentrate on establishing, funding and operationalizing such plans. This will go a long way in facilitating science and evidence-based decision making. The establishment of a Pan-African medical response team will assist governments to quickly access credible information on the appropriate prevention and treatment responses and on the effects of the virus.
- Leverage crisis to build capacity and infrastructure required for post-pandemic innovation ecosystems. This includes availing innovative testing centers – like the South Korean testing booths – in necessary areas to increase the chance to curtail community infections. We are already seeing prototypes in Nigeria.
- Introduce proposed sanitation and hygienic practices in a contextually relevant way. Allocate adequate resources to isolate, quarantine and monitor all confirmed and suspected cases, both symptomatic and asymptomatic, with the government shouldering costs to encourage citizens to get tested.
*Culture may make it easier to implement these measures in certain countries and make it difficult in others but there must be long term public engagement to secure community buy-in. Access to basic infrastructure should be addressed with disenfranchised communities’ needs addressed as part of a response plan. Local solutions should be sourced and buy-in received before implementation.
- Roll out early economic responses
- Identify and assist the most vulnerable sectors of the economy through safety nets and tailor the intervention to the needs of the intended recipients. There are specific sectors of the economy that are most affected by pandemics and the ensuing measures, such as the informal sector in Africa, gig workers, the aviation sector and the hospitality and tourism sector. Where more people are formally employed, wage subsidies and tax reliefs for companies may be more suitable. For example, Kenya’s US$470 million and South Africa’s US$26 billion stimulus packages.
- Support for leveraging technology and innovation with ethical oversight
Technology is playing a pivotal role in the management of COVID-19 in screening, tracking, tracing and monitoring suspected and confirmed cases to the creation of epidemiological models used to determine the most appropriate measures to take and resource optimization. Digital money transactions and e-commerce are proving to be useful tools in accelerating containment measures. We recommend:
- Medical devices and interventions
- African countries should leverage the ongoing efforts to produce medical devices and protective equipment such as ventilators and face shields to promote local production over imports. The shortage in personal protective clothing was evident in all countries including the major economies, largely because the main supplier, China, was affected and on lockdown. Reliance on old industrial economy models has proved costly and therefore, countries should strive to build manufacturing capacity within. Taiwan was able to create value by investing in 60 new production lines for masks, producing enough for its own use and donating the surplus to other parts of the world. Manufacturing using open source templates can also be done via FabLabs and the maker communities, designers, entrepreneurs.
- African countries should explore the use of drones in logistics and delivery of medical supplies for both speed and ease of access to remote, hard to reach or dangerous areas, learning from Rwanda and Ghana who are using drones for public awareness and delivery of test samples.
- Innovation that improves interagency capacity and collaboration
- Develop integrated platforms to enable real-time sharing of critical information between agencies, allowing more agile responses. Taiwan integrated their databases which enabled better coordination between different government agencies and swifter responses in time-critical scenarios. Governments should invest in the necessary hardware and software infrastructure, applications, analytics tools and human capital while ensuring that data governance policies and procedures are in place and where necessary allow open access to the data for researchers.
- Education and Public Engagement
- African countries should shift focus from basic digital literacy to supporting advanced digital literacy competencies. This requires an ongoing review of blended learning models and what would be required in terms of last-mile infrastructure and initiatives, teacher development and measures to respond to growing inequality. As an immediate measure, we recommend the government look to successful Edtech solutions in countries like Kenya, South Africa, Egypt and other emerging economies for expansion in their countries.
- Support Art-Science partnerships and collaborations to provide innovative approaches to raising awareness and impacting human behavior. According to medical experts, the best way to stop an outbreak may lie more in behavioral science than in medical science, therefore, there is need to explore further the role citizen science can play in bridging this gap, for example, initiatives by Senegalese artists.
- Produce pandemic response information in local languages to ensure that the entirety of the population is able to understand the magnitude of a pandemic as well as the preventive measures.
- Improving informed consent. Various countries have adopted surveillance technologies to track and trace travel patterns, but these invasive practices, though necessary, intrude on personal privacy and there are fears in some quarters that after COVID-19 these same practices may continue unabated. This shows that there is a delicate balance between rights and responsibilities in the midst of a global public health crisis, therefore, it is crucial to probe what the trade-offs are and have public consultations on proposed measures.
Download the opinion paper here!
Lead Author: Dr. Youssef Travaly, Vice-President
Additional Authors: Aretha Mare, Research Officer and Esther Kunda, Policy and Innovation Manager
Editor: Nathalie Munyampenda, Managing Director
[1]Point de Situation Pandemie de COVID 19 au 28/04/2020 (ISAO,2020)
[2] Significant clusters are areas with a minimum of 10 cases that are connected through transmission but from different households.